
Injury Surveillance and Injury Prevention in High-Performance Settings
Filippo Siragusa, Physiotherapist, OMT, CSCS
In a context like the NBA, the athlete is not only a technical performer in the game but also a highly valuable strategic asset, with significant implications on the sporting, economic, and organizational levels. Their availability to play is a crucial variable for the competitive balance of the franchise, influencing the season's progression and guiding decisions related to management, logistics, and investments.
An injury does not simply result in a missed performance but triggers a domino effect, redistributing workloads within the roster, compromising the quality and effectiveness of collective performance, and potentially impacting motivational and relational factors within the team (1) . For this reason, over the years, increasingly sophisticated tools have been developed to quantify the actual impact of injuries, with particular attention to performance dimensions.
Among the most used metrics in professional settings are indicators like Games Missed, which represents the total number of games missed by injured players; Injury-Adjusted Wins, an estimate of the theoretical victories that could be achieved without injuries; Win-Loss Differential with Injuries, which measures the difference in the team's performance with and without key players; and Player Availability Impact on Team Performance, a parameter that evaluates the impact of absences on overall performance, using indicators like Net Rating or offensive and defensive ratings.
In this context, managing a professional athlete in a high-intensity environment like the NBA is focused on two main goals: optimizing availability to play during crucial phases of the season and preserving the longevity of athletes’ careers.
From this perspective, sports epidemiology plays a central role. Not so much in terms of systematically collecting data, but rather in interpreting it rigorously and without distorsions, so that it becomes a source of knowledge useful to support shared clinical, managerial, and strategic decisions.
Data only gains value when it allows for context reading, understanding risk dynamics, and guiding targeted interventions through a proactive approach capable of questioning historically consolidated paradigms (2).
Basic epidemiological knowledge thus constitutes the first level of understanding from which a generic risk estimate can be derived (a so called generic warning index) related to practicing a certain discipline, a specific tactical role, or a particular level of competitive exposure. This knowledge allows for identifying the most frequent issues, building a competitive advantage based on the ability to anticipate problems and allocate resources to the most relevant areas (3).
One of the key references for understanding the practical application of injury surveillance is the Translate Reaserch into practice TRIPP model (4). This framework emphasizes that it may not be enough to demonstrate that an intervention works under ideal conditions, but it is crucial to assess its real applicability and sustainability within the operational context of a complex sports organization, like an NBA franchise.
The model is articulated in several interdependent phases: identifying the problem quantitatively,analyzing risk factors and injury mechanisms, designing the preventive intervention, and finally, implementing it within the system.

(Finch 2006)
Injury surveillance is the foundation of this entire process. Only through solid, systematic, and integrated data collection can contextual knowledge be generated to fuel informed and timely decisions.
In an environment like the NBA, optimizing the information derived from Injury Surveillance means integrating clinical data with performance, load, and subjective perception data to gain a multidimensional view of the athlete's state in order to manage different kind of injuries.
It might be useful to have dynamic, intuitive, and real-time updatable dashboards that provide key indicators easily interpretable by all members of the technical, medical, and performance staff.
The analysis of the information gained may focus on early signals and recurring patterns, aiming to anticipate issues before they manifest (feedforward), moving beyond a purely retrospective approach (feedback). In this way, management strategies can be personalized or at least scheduled based on similar clusters, and ideally adapted to the specific characteristics of each athlete.
The ultimate goal should not be a sterile quantitative monitoring but the transformation of information into action.
From a descriptive analysis, it is desirable to reach an analytical interpretation capable of generating coherent, adaptable, communicable, and, above all, sustainable interdisciplinary interventions in the long term.
In this perspective, injury surveillance is not just a technical function, but a strategic lever to maximize efforts aimed at optimizing the availability and performance of the entire team throughout the season.

IOC Consensus (2020)
Key Elements Of Injury Surveillance
How can we define, record and report an injury?
One of the key aspects for effective injury surveillance in the NBA is the precise definition of what constitutes an "injury" and how it is recorded and reported. According to the IOC Consensus 2020 (5),a sports injury is defined from an epidemiological perspective as "any event that results in a change in the physical or mental health status of an athlete, arising from sports activity, that affects their availability to participate in subsequent sporting activities." This broad definition allows for the inclusion of both injuries that result in actual absence and those that, while not preventing participation, negatively impact performance.
Despite the attempt to harmonize language through international consensus, differences related to the context and perception of the term "injury" remain, varying depending on the stakeholders involved (6), who tend to assess its impact primarily on performance.
From a purely biological perspective, however, an injury is described as the result of a situation where a load (either acute or cumulative) exceeds the tissue's adaptive capacity, causing structural or functional damage (7).

The very essential prerequisite for the quality of injury surveillance is the standardization and systematic collection of data. This involves, among other things, deciding in advance which approach to adopt: a "narrow" definition, which considers only injuries leading to absence from activity ("time-loss injuries"), or a "broad" definition, which includes all events requiring medical attention, even without loss of availability ("medical-attention injuries") (8) (9).
The IOC Consensus promotes terminological clarity and uniformity in the collection of epidemiological data, suggesting shared recording methods that facilitate comparability between studies and contexts. This includes the measurement of key variables such as incidence, severity, prevalence, and burden, as well as the monitoring of recurrences, description of injury mechanisms (e.g., contact vs. non-contact), and the use of standardized diagnostic coding systems such as OSICS (5).

(Impellizzeri et al., 2022)
A clear terminology is also crucial in relation to other central concepts such as return to play, exposure, availability (complete or partial), incidence (number of new cases in a given period), and prevalence (total number of cases at a specific time). These metrics, often subject to misinterpretation, require greater attention (10).
A retrospective analysis of an NBA injury database, including the pandemic period, highlighted that the lower extremities — particularly ligament and tendon structures — are the most frequently affected anatomical sites. Guard and point guard roles are the most exposed, likely due to high minutes played and a playing style characterized by rapid and explosive actions. The study also reports that most injuries occur in the second half of the regular season and that less experienced players tend to be more vulnerable, possibly due to a lack of awareness in load management or immature playing characteristics (11).
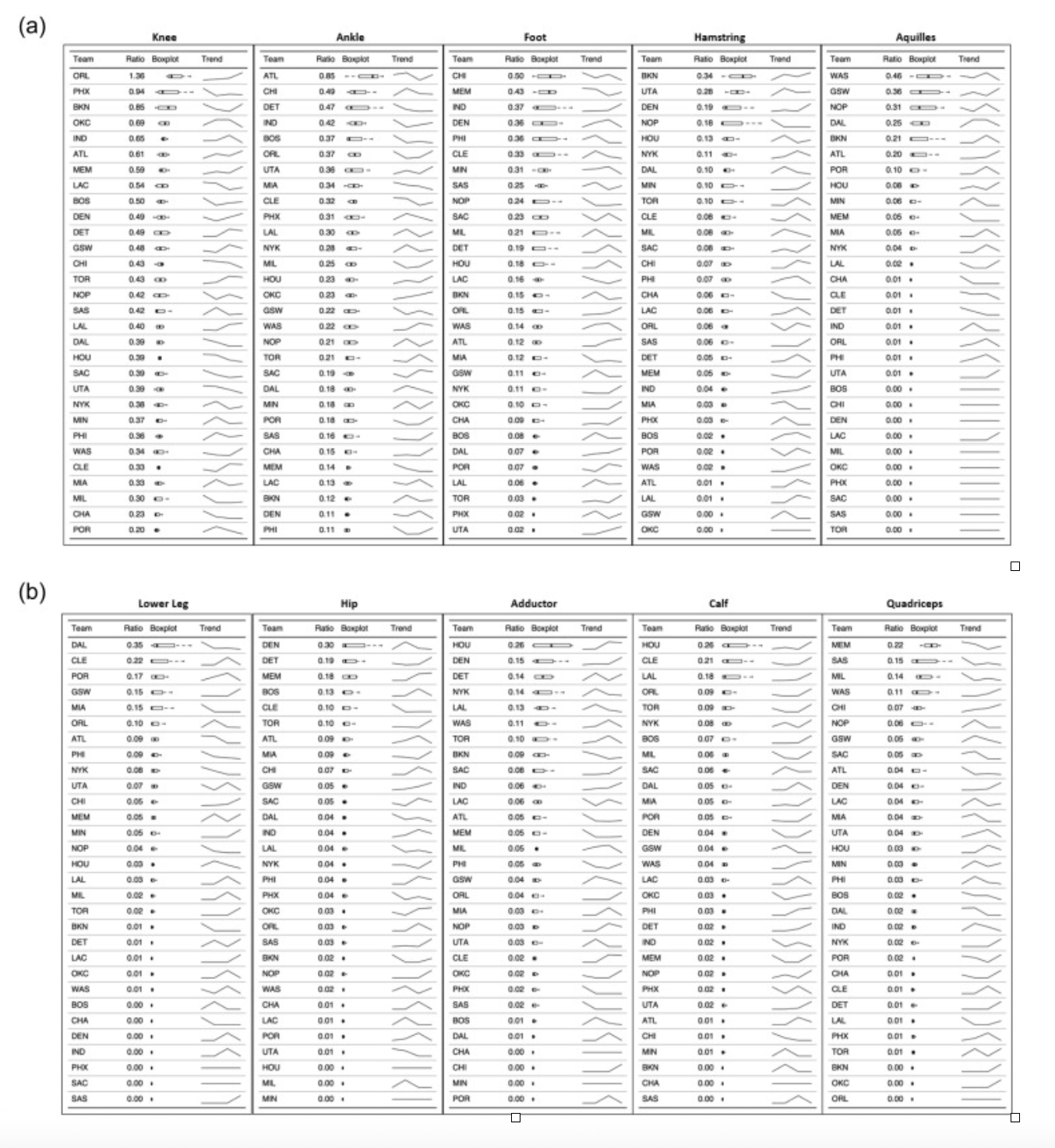
(Torres Ronda 2022)
These data show that even within the same league and season, heterogeneous risk patterns can coexist. Some teams, for example, may register specific trends or high prevalence of certain injury types, while being less affected by others. This reinforces the need for a contextualized epidemiological reading that can be adapted to the specific needs of each team.
It should also be emphasized that, to date, the NBA does not have an official, centralized platform for the collection and dissemination of epidemiological data, unlike what happens in other sports or federations (12). Moreover, there are no specific extensions (such as in gymnastics, soccer, ski and so on..) of the IOC guidelines adapted to the peculiarities of basketball and its situational pattern, which could instead help improve the quality of data collection and analysis systems according to sport-specific logic.

(Van Mechelen 1992)
Understanding Risk
What’s your risk tolerance?
The study of sports injury prevention has evolved significantly over time, transitioning from a linear and simplified approach to a more complex, dynamic, and interactive view. Over the years, various theoretical models have been developed with the aim of understanding the risk of injury as a multifaceted phenomenon, capable of integrating different perspectives and more sophisticated methodological approaches.
In 1992, a systematic and linear model for prevention was proposed, with the merit of clearly structuring the entire process: from defining the problem, identifying risk factors, to implementing and evaluating preventive strategies. However, despite its utility and applicability, this model had some limitations, particularly in not considering the complexity of interactions between various factors, treating them as isolated and static entities, and overlooking the dynamic evolution of relationships over time.
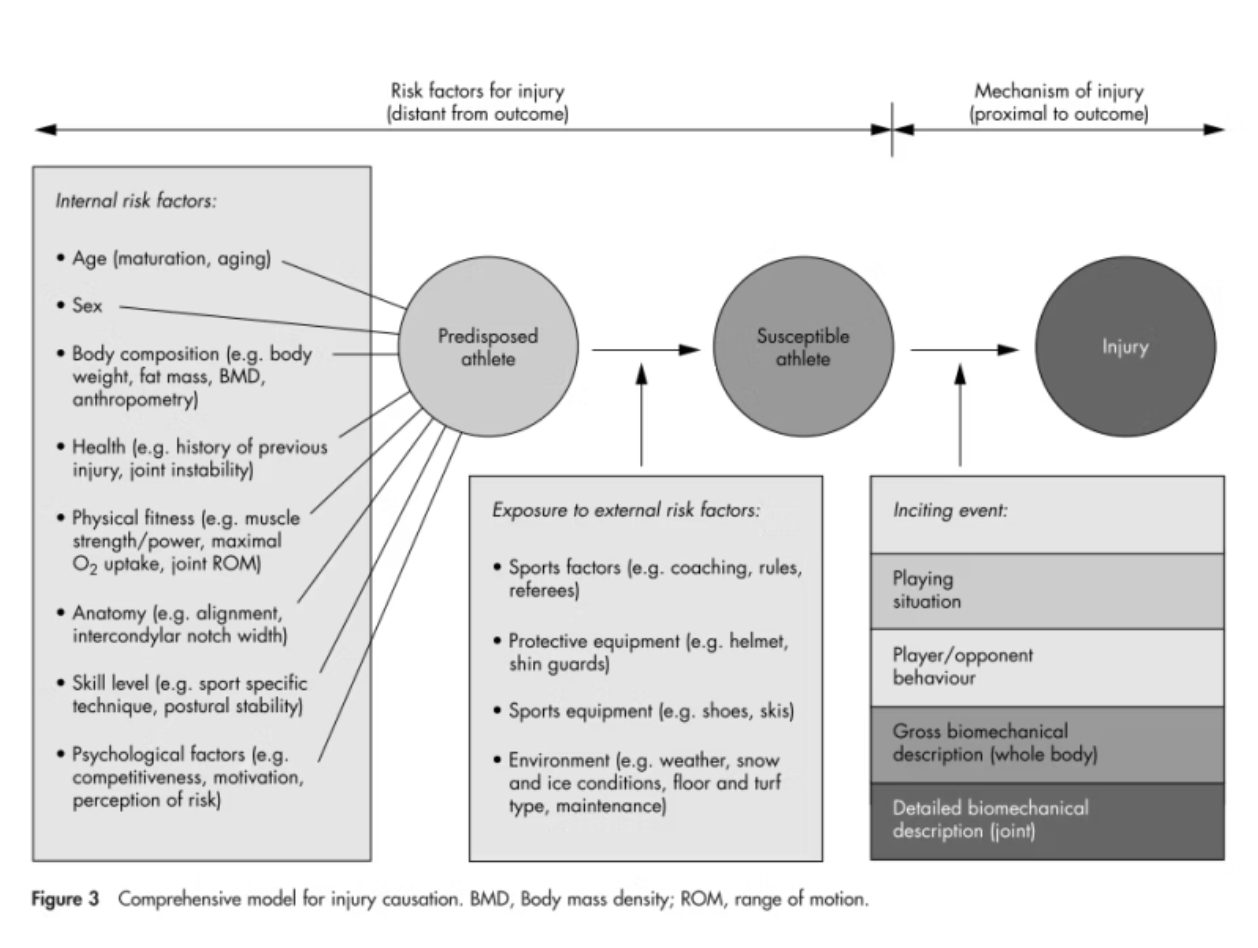
(Meuwisse 2006)
In 2006, a multifactorial perspective was introduced, integrating intrinsic — both modifiable and non-modifiable — and extrinsic factors, linking them to potential triggering events. Although more detailed, this approach remained anchored to a static view, not fully considering how interactions between factors could evolve over time and in different contexts.
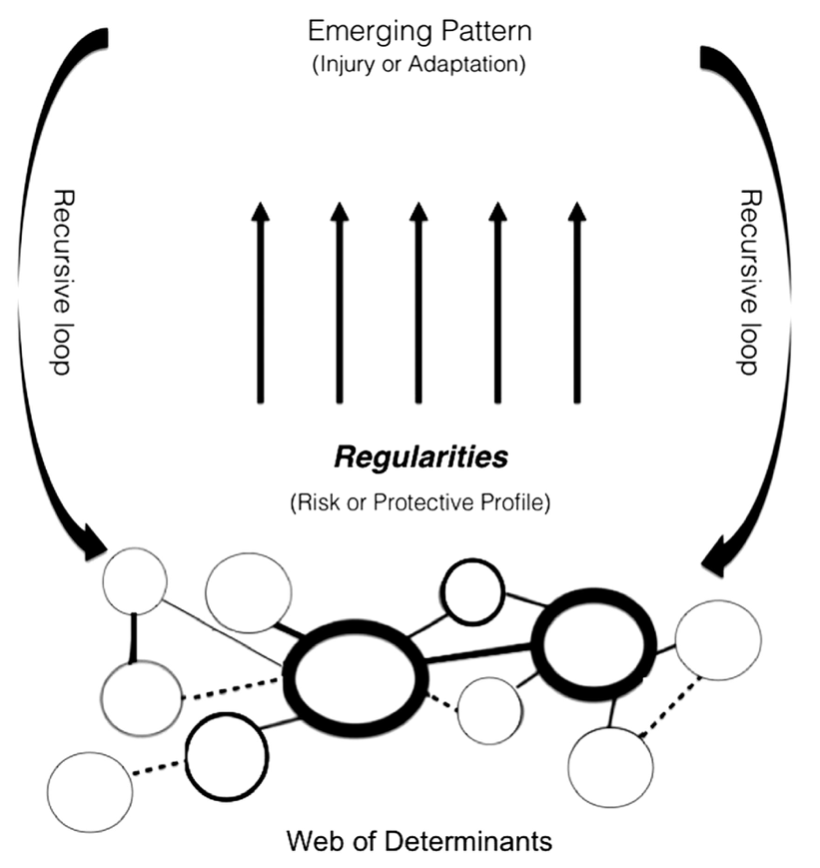
An additional evolution came with the complex systems approach, according to which the risk of injury emerges as the result of a dynamic system, where small variations in one or more factors can generate disproportionate effects. Risk is therefore not a simple sum of elements, but the outcome of continuous and evolving interactions. From this arises the need for flexible and adaptable preventive strategies, capable of responding in real time. Injury risk thus takes the form of a process where past conditions influence future ones according to feedback and adaptation dynamics (13).
When assessing the effectiveness of preventive measures, it is essential to consider their real, not just theoretical, impact. There is no one-size-fits-all approach; rather, there are tailored interventions adapted to individual characteristics. In this sense, different response profiles can be identified:
Doomed: Athletes with genetic predispositions or structural vulnerabilities who do not respond effectively to prevention. For them, the goal is not to eliminate the risk but to manage it, improving quality of life and career.
Immune (or Survivors): Naturally protected players for whom preventive strategies may have less impact but are still beneficial.
Preventive: Athletes who significantly benefit from interventions, reducing risk through targeted programs.
Causal: Individuals who get injured despite preventive measures, due to negative adaptations or side effects of the same interventions (14).
To fully understand the risk of injury, it is necessary to distinguish between risk factors, injury mechanisms, and concepts of causality. Causality is assessed by considering criteria such as temporality (the factor must precede the injury), intensity of the link, dose-response relationship, consistency of the results, and adherence to theory. Specificity, however, is very rarely observed, as sports injuries are multifactorial.
Risk factors are conditions that increase the probability of injury but manifest far from the actual injury event. Their identification requires prospective studies with large samples.
Injury mechanisms, on the other hand, represent the immediate events leading to the injury and can be studied through interviews, video analysis, instrumental tests, and biomechanical assessments (15).
A useful example can be extrapolated from these works on the Achilles tendon rupture, that examine the relationship between previous injuries and ruptures (ATR) in NBA players, highlighting that players over 30 with a history of Achilles or lower leg injuries have a 4 times higher risk (16) and how biomechanically, ruptures occur during explosive movements (jumps, direction changes), especially in situations like false steps or the first offensive step, with high eccentric loads and neuromuscular fatigue (17).
While 2D video analysis and the retrospective may give a few more cases to for the analysis, the approach have limitations, they must be balanced with the practical difficulty of integrating field observations and 3D laboratory analyses. Bridging this gap remains a central methodological challenge.

(Verhagen 2024)
More pragmatic considerations may shift the focus from simple risk reduction to dynamic management based on the concept of tolerance thresholds. In high-intensity environments like the NBA, where high loads and tight schedules are inevitable, it becomes essential to distinguish between acceptable and unacceptable risks.
This requires classifying injuries not only by frequency but by severity and burden, prioritizing interventions for those with high performance and economic impact. More aggressive strategies should be established for preventing "catastrophic" injuries, while allowing greater exposure to minor injuries. Risk thresholds should be adapted to the strategic value of the athlete, the phase of the season, and the context, in an interdisciplinary perspective.
The goal is not to eliminate every injury but to make informed decisions about which risks to take, transforming prevention into a strategic lever for performance while accepting the often inevitable trade-off between maximizing performance and the residual risk of injury. (18)
Injury Surveillance and Injury Prevention
Find an ally that can help you to optimize your resources
In highly competitive contexts like the NBA, where every game matters and the seasonal load tests every aspect of preparation, player availability is one of the most crucial variables for success. With over 80 regular-season games, relentless travel, back-to-back games, and high performance pressures, the concept of injury prevention goes far beyond simply avoiding injuries. The real challenge is broader: reducing risk, managing uncertainty, and building a system that is sustainable over time, capable of protecting athletes' health without compromising competitiveness.
Within this system, injury surveillance may become a sort of map that guides clinical, technical, and managerial decisions. The systematic collection of data on injuries and loads — training, games — provides a clear view of the real burden of the season. Effective surveillance allows us to quantify the incidence and severity of injuries, identify recurring patterns during critical moments of the schedule, the impact of coaches’ styles, recognize athletes or contexts at high risk, and evaluate the effectiveness of interventions.
Talking about prevention it’s essential to distinguish between three levels, each with a defined role in the NBA workflow.
Primary prevention focuses on reducing risk from the start, through structured programs for strength, motor control, technical progressions, and recovery management. The main challenge here is not so much the design of interventions, but their implementation: adaptability, sensitivity to context, and a constant balance between theoretical effectiveness and daily practicality are required. Optimizing time as one of the best resource and Implementing lab-based concepts in the real world can be complex since the literature in sports physiotherapy provides few specific guidelines for highly specialized contexts like the NBA (19).
Secondary prevention focuses on early interception, recognizing initial signs of overload or discomfort before they lead to full injuries. This requires constant attention to subjective data, such as perceived fatigue, muscle soreness, or sleep quality, as well as a careful reading of fluctuations in performance tests. Small signals, such as a decrease in stiffness, emerging asymmetry, or a reduction in jump quality, when interpreted promptly, allow for intervention before the problem becomes clinical (20), this approach rely more on the understanding of what’s the current state of the athlete, rather than find an univocal cause.
Tertiary prevention comes into play when the injury has already occurred, aiming to promote functional recovery (21), prevent the risk of recurrence, and allow for a return to competition based not only on physiological criteria but also contextual ones. In this process, communication and alignment between physiotherapists, doctors, sports scientists, and coaching staff are essential. Every decision has significant consequences, and interdisciplinarity is not just an added value, but a necessary condition to ensure that the return to the field is sustainable (8) (22).
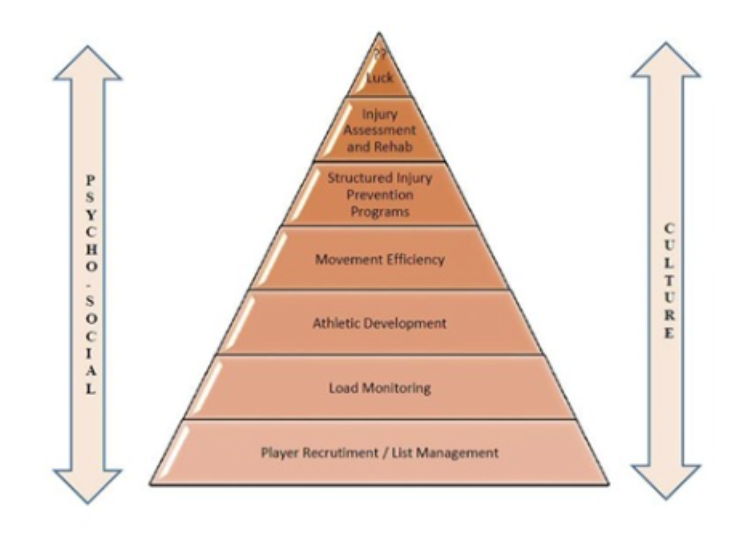
(Coles 2016)
Looking at the entire system, prevention can be seen as a pyramid structure. At the base, we find organizational culture, often an invisible but crucial element. Without an environment that genuinely prioritizes the health of athletes as a shared priority, no intervention will be truly effective (but you can say it’s a part of the business). This implies creating a climate of trust, clear communication, and constant alignment among those making technical, medical, and managerial decisions. A solid foundation allows for the construction of the subsequent levels. Operational processes — such as the aware use of technology, smooth data sharing, load management, and periodic assessments — become key tools for translating values into concrete actions. With solid foundations, technical interventions – exercises, treatments, biomechanical modifications, recovery strategies – fully express their potential (23).
(Bolling 2019)
But the real breakthrough may reveal conceptual: we need to move beyond the checklist mindset and embrace a wider approach. Injuries are never the result of a single mistake or a single gap, but the outcome of a complex web of interactions between physical, psychological, organizational, environmental, and relational factors. Therefore, thinking about prevention means conceiving it as an adaptive system, made up of connections, communications, and continuous adjustments.
In the daily work with an NBA team, the real challenge is not simply deciding "which test to do" or "which exercise to propose," but how to ensure coherence between strategy, communication, operations, and context.
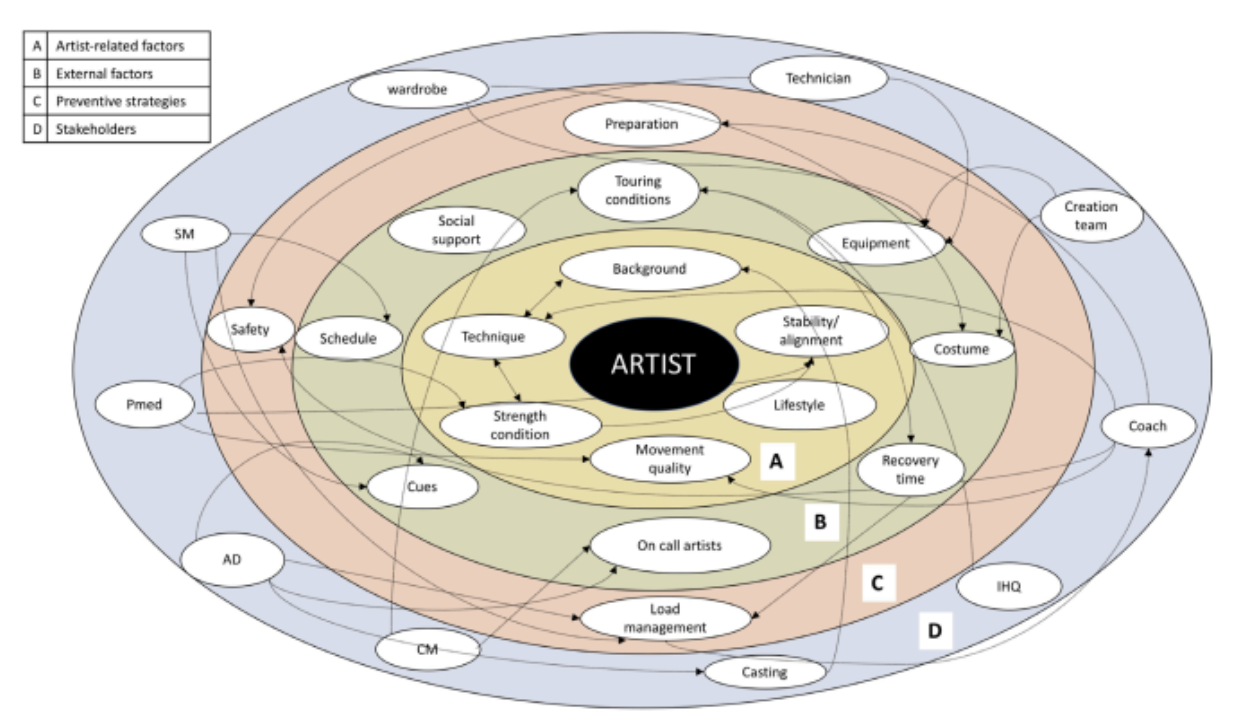
In this ecosystem, athletes, physiotherapists, athletic trainers, doctors, performance analysts, coaching staff, and management interact constantly. But it’s not just about roles: daily habits, decision-making processes, expectations, and the atmosphere in the locker room come into play. Every element can influence the others, amplifying or reducing risk. That’s why conceiving prevention as an ecosystem means being able to read invisible connections, anticipate imbalances, and promote a culture of continuous dialogue. Only by doing so can we create an environment that truly protects the long-term availability of the athlete. Ere an example from the Cirque Du Soleil (24).
Understanding the Context

(Bolling 2018)
That’s where your soft skills can make a difference!
In the NBA, where athlete performance is closely tied to physical availability, IS plays a crucial role. However, data reliability remains a constant challenge: beyond objective measurements, it is essential to integrate subjective data provided by the athletes themselves, such as perceptions of fatigue, pain, and stress. The ability to understand the athlete’s experience and context can be crucial (25).
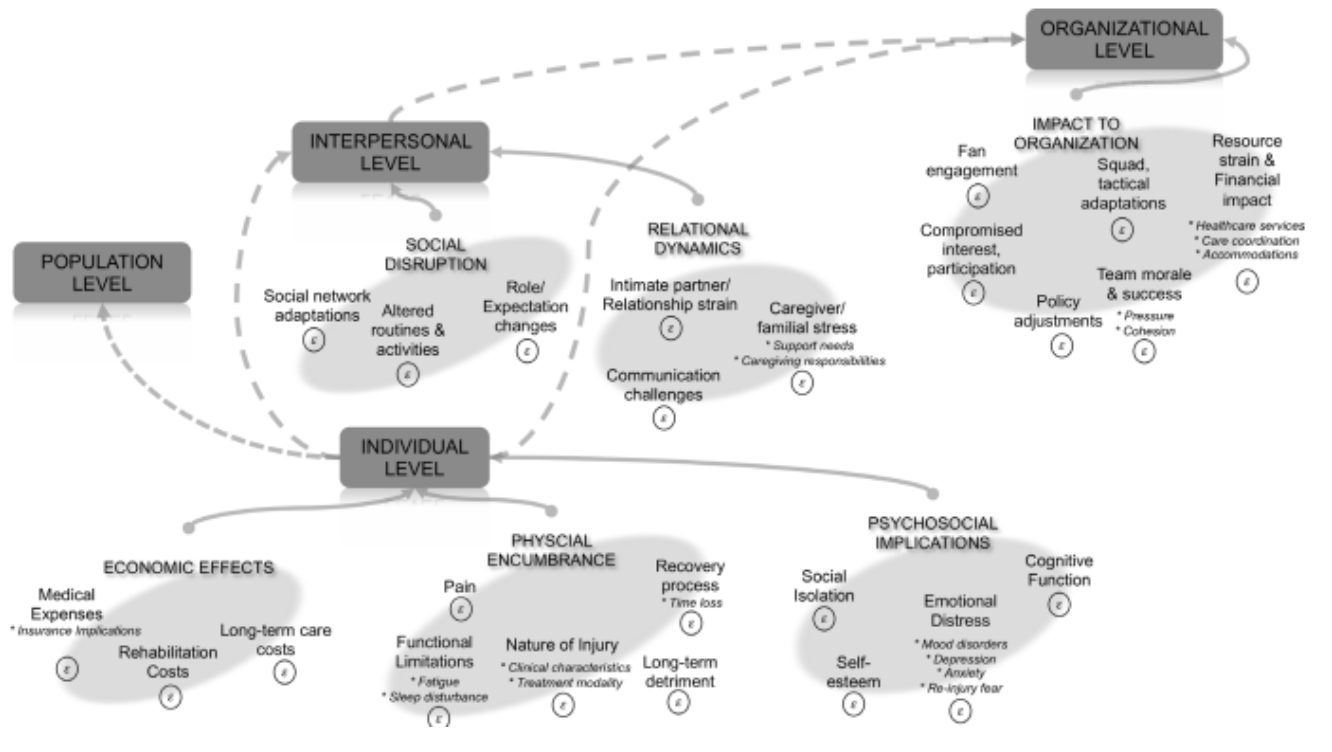
Beyond purely biological, biostatistical, or biomechanical dimensions, a key insight in recent years has been the need for a reflective approach to injury and its reporting—one that considers not only the physical component but also the psychological, social, and professional dimensions. A simple epidemiological burden measure is no longer sufficient to represent the real impact of an injury: a broader model is needed, one that captures its full complexity (26).
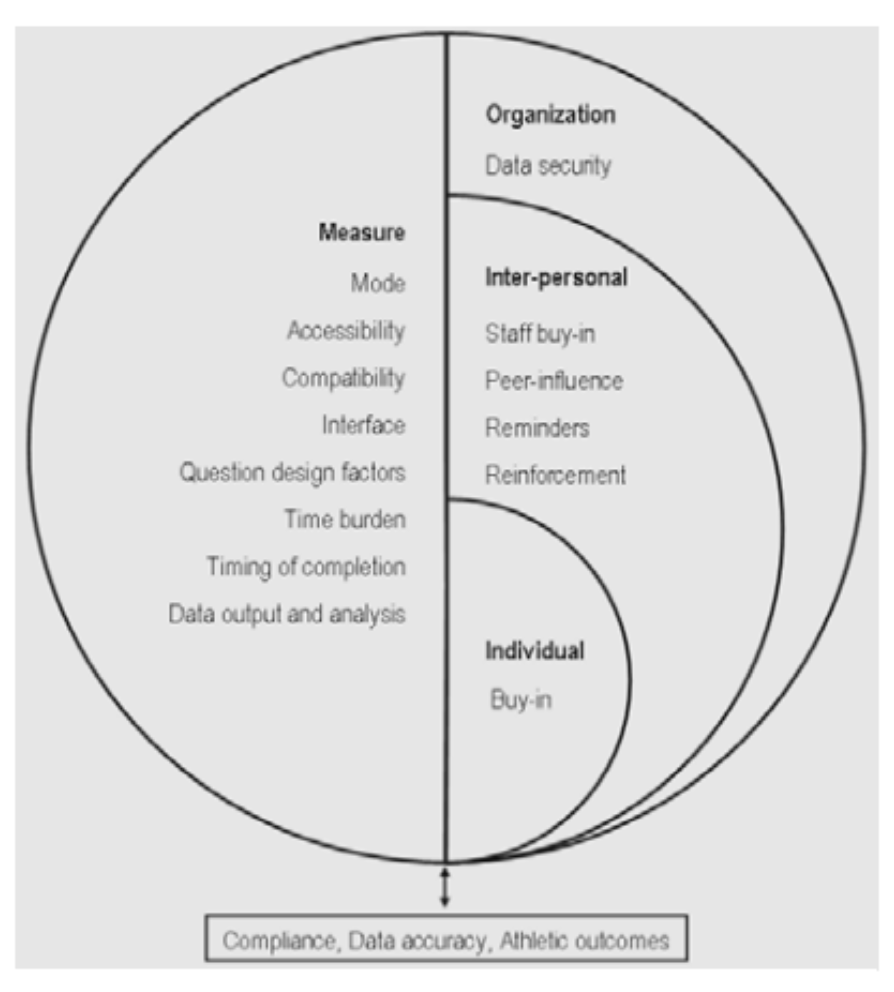
As highlighted by several studies, subjective data (self-reports) and health status feedback are valuable tools, but they are vulnerable to bias. It is common practice for athletes to “pretend to be fine” to avoid being excluded from the rotation, or to “pretend to feel worse” to gain rest or a reduced workload. The quality of this data strongly depends on the relational culture between athletes and staff: an environment that fosters trust and transparency significantly reduces these dynamics (27).
(Saw 2015)
Integrating subjective data with objective measurements — for example through wearable technologies — is an effective strategy to compensate for individual biases and achieve a more reliable and comprehensive view. However, for IS to be truly effective in the NBA context, an organizational culture that supports two-way communication and actively involves athletes, doctors, strength coaches, and head coaches is required.
Beyond relational aspects, it’s important to recognize that the NBA playing style is constantly evolving: increased pace, greater spacing, the extension of shooting range, and a rise in high-speed transitions have redefined the physical demands on athletes. These changes require a contextual reinterpretation of epidemiological data, moving beyond a static view of injury surveillance toward a more dynamic and adaptive approach. For instance, a team like the 2014–2015 Houston Rockets, once considered extremely perimeter-oriented, would now rank 29th out of 30 in three-point attempts (28).
Just as coaches must adapt to the evolution of the game, clinicians must understand changes in performance models to develop preventive strategies that align with the contemporary reality of the league. The new emphasis on perimeter play, the extended operational range even for big men, and the increase in high-intensity sprints and direction changes have altered the predominant biomechanical profile compared to just a decade ago.
The real challenge therefore is not only in data collection, but in translating data into communicative and operational tools that are understandable and usable in practice. Data must speak the language of performance. A player is more likely to follow a rehab protocol if they understand it will help them return to the court faster and perform better, rather than for a generic health principle. Communication must be contextualized, targeted, and “performance-oriented”, you might think think coaches and athletes as more instinctive animals (like felines), and clinicians and sport scientists to more rational ones (like monkeys).
Likewise, coaches and strength staff need clear, actionable information. A periodic report should not be a complicated table, but a practical suggestion: “can do plyometrics” or “reduce change of direction drills.” In a high-performance system, IS must become a daily extension of the decision-making process and respond to basic stakeholder needs, such as: “what’s in it for me?” (29).
In the end, what matters is not how much data we collect, but how well we are informed and how we translate it into tangible competitive advantages: more minutes played by our best athletes, more consistent performances throughout the season, and longer, more successful careers.
Probably, the true success of sports medicine in the NBA is measured by its ability to bridge the gap between scientific complexity and the immediate demands of elite sports.
With this in mind, interdisciplinarity represents a crucial evolution: it does not simply add together different competencies (as in the multidisciplinary model), but integrates them into a coordinated system where specialists from different fields — medicine, strength & conditioning, psychology, data analysis — collaborate actively with shared goals.

(Salcinovic 2022)
This approach requires structured communication, mutual trust, and strong leadership capable of orchestrating teamwork and ensuring coherence between technical, medical, and strategic decisions. The performance coordinator plays a central role in facilitating alignment across the staff, ensuring a shared operational language, and keeping the athlete at the center of decision-making.
Breaking down silos, reducing communication barriers, and fostering a culture of continuous dialogue are essential conditions to manage the complexity of the modern game and effectively respond to challenges related to athlete health, workload, and availability (30) (31).
To generate real impact, IS must be systemically integrated into the team's organizational workflow. Constant collaboration between performance staff, medical area, and coaching staff is essential. Monitoring must become a daily habit, not an exceptional action.
Practical Implications:
Differentiated monitoring: athletes with a history of tendinopathy should undergo regular ultrasound screenings and biomechanical assessments.
Smart load plans: training volumes and minutes must be modulated based on individual risk factors.
Active prevention: specific strengthening and mobility programs to address post-injury asymmetries.
Ethical and Privacy Considerations: Due to the invasive nature of some monitoring techniques, there's an increased emphasis on data privacy, ethical considerations, and adherence to data protection regulations.
The real success metric of a preventive program should remain availability, sometimes even if an athlete may result clinically healthy but not optimally available. Maximizing availability means not only reducing injury incidence, but also optimizing the use of resources during key moments of the season (1).
Example of interdisciplinary approach for AT injury in a high risk profile athlete with recurrent lower leg injury:
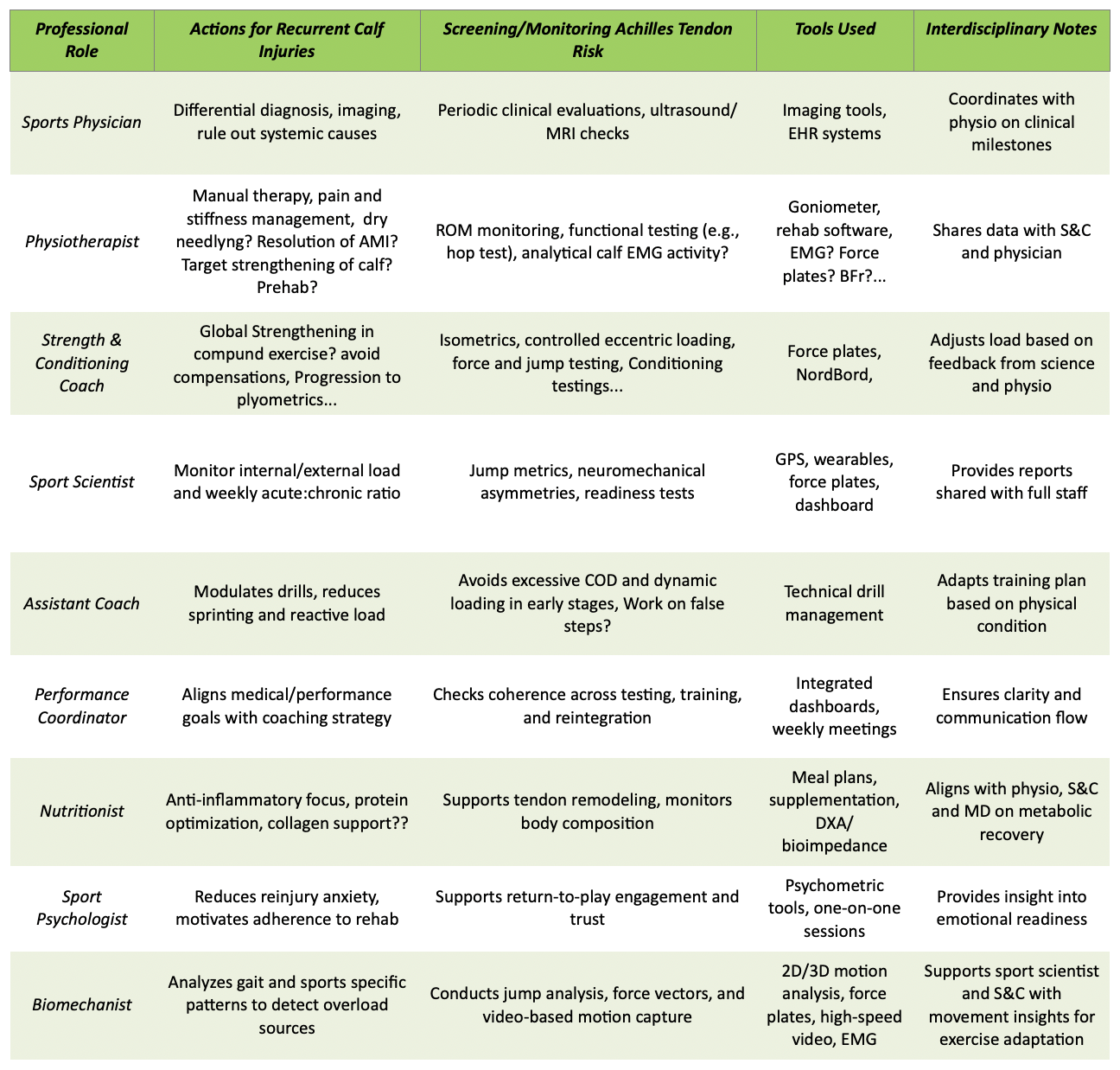
(PLEASE consider this as a very general example, contexts may be very different)
Future Developments
Look ahead but don’t forget what you did well
The introduction of artificial intelligence and predictive models is revolutionizing injury prevention in the NBA, but it is still crucial to distinguish between association and causality since while machine learning can identify correlations, it does not imply a causal relationship therefore drawing conclusions from a bunch of data recorded, based solely on these correlations can lead to incorrect decisions.
Another key aspect is model validation. Without proper validation, models that shoulde be supposed to inform our decisions can suffer from overfitting and may not be applicable in new contexts. They need to be both accurate and generalizable to be truly useful.
Moreover, it is essential that models are interpretable, understandable and useful for professionals, such as coaches and sports doctors, and not just a "black box." (32)
In this context, the physiotherapist may acquire the skill to be a "data translator," able to combine data with clinical insight. Although wearable devices are widespread, their ability to predict injuries remains controversial. At the moment they should probably be used for load monitoring, not as predictive tools.
In the future, the evolution of surveillance systems must not only focus on collecting more data, but on making that data meaningful since data collection and use will be more integrated, standardized, and shared across different levels - from NCAA teams to NBA franchises- and across different sports.
More accessible technologies, such as software and mobile apps, will make injury surveillance more widespread, but the goal will remain to transform data into insights to improve athlete health, performance, and longevity using our clinical and rehabilitation skills (33).
References
1. Windt J, Ekstrand J, Khan KM, McCall A, Zumbo BD. Does player unavailability affect football teams' match physical outputs? A two-season study of the UEFA champions league. 2018.
2. team, The Barça Innovation Hub. https://barcainnovationhub.fcbarcelona.com/blog/how-the-epidemiology-of-injuries-can-help-to-better-understand-and-manage-injuries-in-professional-basketball/. [Online]
3. David Joyce, Daniel Lewindon. Sports Injury Prevention and Rehabilitation. Abingdon, Oxon ; New York, NY : Routledge, 2016.
4. C, Finch. A new framework for research leading to sports injury prevention. J Sci Med Sport. 2006.
5. R, Bahr. International Olympic Committee Consensus Statement: Methods for Recording and Reporting of Epidemiological Data on Injury and Illness in Sports 2020 (Including the STROBE Extension for Sports Injury and Illness Surveillance (STROBE-SIIS)). Orthop J Sports Med. 2020.
6. Bolling, Barboza, van Mechelen, Pasman. How elite athletes, coaches, and physiotherapists perceive a sports injury. Translational Sports Medicine. 2019.
7. Wang C, Stovitz SD, Kaufman JS, Steele RJ, Shrier I. Principles of musculoskeletal sport injuries for epidemiologists: a review. Inj Epidemiol. 2024.
8. M., Whalan. https://www.sportsmith.co/articles/how-to-build-a-programme-to-minimise-injuries/. Sportsmith. [Online]
9. al, Clarsen B et. Improved reporting of overuse injuries and health problems in sport: an update of the Oslo Sport Trauma Research Center questionnaires. Br J Sports Med. 2020.
10. Impellizzeri FM, McCall A, Meyer T, van Smeden M. Measures of (injury and illness) occurrence: a primer on epidemiological concepts and terminology for authors. Sci Med Footb. 2022.
11. Torres-Ronda L, Gámez I, Robertson S, Fernández J. Epidemiology and injury trends in the National Basketball Association: Pre- and per-COVID-19 (2017-2021). PLOS One. 2022.
12. Costello, D., Daly, E. e Ryan, L. Sports Injury Surveillance Systems: A Scoping Review of Practice and Methodologies. J. Funct. Morphol. Kinesiol. 2024.
13. Bittencourt NFN, Meeuwisse WH, Mendonça LD, Nettel-Aguirre A, Ocarino JM, Fonseca ST. Complex systems approach for sports injuries: moving from risk factor identification to injury pattern recognition-narrative review and new concept. Br J Sports Med. 2016.
14. Shrier I, Impellizzeri FM, Stovitz SD. Prevention versus risk reduction or mitigation: Why create unnecessary battles? . J Sci Med Sport. 2023.
15. Verhagen, Van Mechelen. Injury Sports Research. s.l. : Oxford, 2013.
16. Petway, A. J., Burch, R. F., Saucier, D., Gillen, Z. M., Epsley, S., Forbes, R., King, J. Examining prior injury relative to Achilles tendon ruptures in National Basketball Association players. Research in Sports Medicine. 2025.
17. Petway AJ, Jordan MJ, Epsley S, Anloague P. Mechanisms of Achilles Tendon Rupture in National Basketball Association Players. J Appl Biomech. 2022.
18. Verhagen E, Clarsen B, van der Graaff L, Bahr R. Do not neglect injury severity and burden when assessing the effect of sports injury prevention interventions: time to paint the whole picture. Br J Sports Med. 2024.
19. Nimphius, S., & Kadlec, D. A warm-up is not a workout: A principles-based critique of continued efforts to use warm-up programs for ACL injury prevention. OSF. 2025.
20. Schusster J, Bove D. Jumping Towards Best-Practice: Recommendations for Effective Use of Force Plate Testing in the NBA. Sport Performance & Science Reports. 2020.
21. Maestroni L, Turner A, Papadopoulos K, Sideris V, Read P. Total Score of Athleticism: Profiling Strength and Power Characteristics in Professional Soccer Players After Anterior Cruciate Ligament Reconstruction to Assess Readiness to Return to Sport. Am J Sports Med. 2023.
22. I., Shrier. Strategic Assessment of Risk and Risk Tolerance (StARRT) framework for return-to-play decision-making. Br J Sports Med. 2015.
23. PA, Coles. An injury prevention pyramid for elite sports teams. Br J Sports Med. 2018.
24. Bolling C, Mellette J, Pasman HR, van Mechelen W, Verhagen E. From the safety net to the injury prevention web: applying systems thinking to unravel injury prevention challenges and opportunities in Cirque du Soleil. BMJ Open Sport Exerc Med. 2019.
25. Bolling C, van Mechelen W, Pasman HR, Verhagen E. Context Matters: Revisiting the First Step of the 'Sequence of Prevention' of Sports Injuries. Sports Med. 2018.
26. Chandran A, Anderson T, Post EG, Kerr ZY, Adams WM. Contemporary reporting in sports injury epidemiology: choosing words carefully and considering a Holistic Injury Impact Framework. Br J Sports Med. 2025.
27. Saw AE, Main LC, Gastin PB. Monitoring athletes through self-report: factors influencing implementation. J Sports Sci Med. 2015.
28. Goldsberry, Kirk. Hoop atlas: mapping the remarkable transformation of the modern NBA. New York : Mariner Books, 2024.
29. Buchheit M. “WANT TO SEE MY REPORT, COACH?”. Aspetar Medicine. 2017.
30. French D, Torres Ronda. NSCA's Essentials of Sport Science. Champaign,IL : Human Kinetics, 2022.
31. Salcinovic B, Drew M, Dijkstra P, Waddington G, Serpell BG. Factors Influencing Team Performance: What Can Support Teams in High-Performance Sport Learn from Other Industries? A Systematic Scoping Review. Sports Med Open. 2022.
32. Bullock, G.S., Ward, P., Collins, G.S. et al. Comment on: Machine Learning for Understanding and Predicting Injuries in Football. Sports Med - Open 10. 2024.
33. et, Sprouse. Injury and illness surveillance monitoring in team sports: a framework for all. Injury Epidemiology. 2024.
About The Author
Filippo Siragusa, Physiotherapist, OMT, CSCS

Orthopaedic Manual Therapy (University of Zaragonza, Spain)
Sports and Exercise Medicine (University of SouthWales, UK)
Biostatistics (University of Padua, Italy)
Fillippo is the father of Riccardo, Matilde and Ludovica, he has worked for six years in the academy of a professional soccer team and has served as a consultant for professional soccer and volleyball players, as well as in the rehabilitation of musculoskeletal and post surgical conditions.
He is currently a subject matter expert for the University of Siena (Italy) and the University of Milan-Bicocca (Monza, Italy), and is an accredited basketball minor league coach with the Italian Basketball Federation.
He has a keen interest in clear and sober clinical communication, strength and conditioning, technology, and data analysis applied to physiotherapy.



